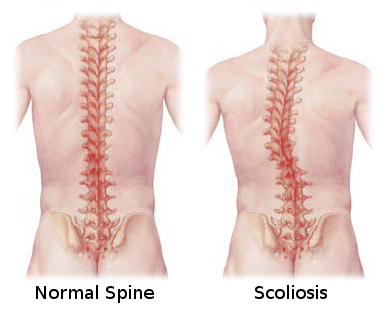
 Scoliosis is a condition in which there is an abnormal lateral deviation of the spine. In layman’s translation: if you look at a person from the back side, the spine has a C-shape or S-shape curve instead of the normal, vertically upright orientation.
Scoliosis is a condition in which there is an abnormal lateral deviation of the spine. In layman’s translation: if you look at a person from the back side, the spine has a C-shape or S-shape curve instead of the normal, vertically upright orientation.
There are two categories of scoliosis: postural scoliosis and structural scoliosis. The purpose of this article is to differentiate these two types of scoliosis, to describe the chiropractic approach to scoliosis care and lastly, to differentiate this from the medical approach. This is so that you may better understand some of the various available options for scoliosis care.
Functional / Postural Scoliosis:
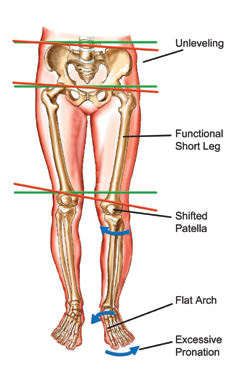 A postural scoliosis is essentially an postural adaptation to an imbalance in your base of support. For example, a leg length inequality or a low arch on one side compared to the other. This will cause the pelvis to dip down on one side. Then your spine will curve as an adaptive response because all of the joints are functionally connected. This type of scoliosis is generally flexible and can be diagnosed from physical examination findings (evidence of short leg and a flexible spinal curve that unwinds with side bending of the torso). This type of scoliosis is also usually fairly straightforward to correct. Custom foot orthotics are used to correct the alignment of the feet or a heel rise is used if there is a structurally short leg. Chiropractic care may also be recommended to the postural scoliosis patient to address any muscle or joint findings and any resulting pain from years of abnormal force distribution.
A postural scoliosis is essentially an postural adaptation to an imbalance in your base of support. For example, a leg length inequality or a low arch on one side compared to the other. This will cause the pelvis to dip down on one side. Then your spine will curve as an adaptive response because all of the joints are functionally connected. This type of scoliosis is generally flexible and can be diagnosed from physical examination findings (evidence of short leg and a flexible spinal curve that unwinds with side bending of the torso). This type of scoliosis is also usually fairly straightforward to correct. Custom foot orthotics are used to correct the alignment of the feet or a heel rise is used if there is a structurally short leg. Chiropractic care may also be recommended to the postural scoliosis patient to address any muscle or joint findings and any resulting pain from years of abnormal force distribution.
Structural Scoliosis:
A structural scoliosis is a bit more complicated to deal with. There are many types of structural scoliosis. One such type is adolescent idiopathic scoliosis. This is a rigid, inflexible spinal curve and for unknown reasons, the spine just grows that way. While the spine continues to grow, there is a risk that it will continue to get worse. Chiropractic management includes manual adjustments and/or mobilizations to the spine to improve flexibility, function, alignment and mechanical balance. Chiropractic care is also helpful for naturally managing pain. Exercises are also prescribed.
Proprioceptive exercises are particularly beneficial for scoliosis patients (of either type). Proprioceptive exercises are exercises that improve body position awareness. Examples include exercises on an exercise ball, rocker board, wobble board or vibration platform. Yoga and Tai Chi are also great balancing exercises. Chiropractic care combined with proprioceptive exercises help to retrain the central nervous system. Beyond this, specific corrective exercises may be prescribed which are designed to stretch the relatively tighter muscles and strengthen the relatively weaker ones. Preferably, these should be done daily. Deep breathing exercises and sleep posture awareness are also beneficial.
Risks of Scoliosis:
Just because you have scoliosis does not guarantee that you will have problems later in life. Many people carry on with their lives with no idea and a scoliosis is incidentally found later. That being said, there are some risks with scoliosis. Statistically, with greater curves there tends to be more pain and also earlier onset of arthritis due to uneven wear and tear to the joints. There is also a risk that the scoliosis may continue to progress (especially during adolescence, when the spine is still growing). With structural scoliosis, there is concern about compression of the internal organs when curves progress beyond a certain point.
Scoliosis Diagnosis:
Scoliosis is diagnosed through physical examination and/or x-ray imaging. The physical examination entails an assessment of posture, flexibility of spinal ranges of motion and orthopedic testing. Chiropractors have trained eyes for detecting posture abnormalities such as unleveling of the shoulders, pelvis, hips, knees and feet which may indicate an underlying scoliosis. If a scoliosis is detected, the second step is to determine if it is postural or structural. A postural scoliosis will unwind upon side bending of the torso. A structural scoliosis will not unwind fully upon side bending and will have a positive Adam’s test (forward flexing the spine will have evidence of rib protrusion on one side). An x-ray may be ordered to evaluate the severity and objectively measure the curve. Other potential causes for scoliosis also need to be ruled out.
Conventional Medical Management of Structural Scoliosis:
The conventional medical management of structural scoliosis involves monitoring, bracing, medication and/or surgery. Medication is suggested only as a means for symptomatic relief and does nothing to solve the underlying cause (which is unknown). If the patient is still growing, progression is monitored by first a baseline x-ray and then follow-up x-rays every few months. If the curve progresses, a spinal brace is typically recommended. A brace is intended to prevent further progression but patient compliance is a challenge because spinal braces tend to be uncomfortable and awkward (especially for the self-conscious adolescent). If the scoliosis progresses beyond a certain point, the patient may be recommended spinal surgery in which a metal rod is surgically fused to the spine to straighten it out. This procedure is invasive and has many inherent risks.
Why Chiropractic Makes Sense:
In light of the other available options, chiropractic care is a logical approach for scoliosis management. Chiropractic care is hands on, non-invasive and drug-free. It attempts to correct the underlying mechanical problems in scoliosis, relieve pain naturally and empower the patient to continue appropriate home care corrective and postural awareness exercises. While there is no guarantee that chiropractic will correct a structural scoliosis, there is evidence in the literature that it can slow the progression and improve the curve in some cases. For these reasons, chiropractic care makes sense. If unsuccessful, the conventional medical management is still an option. While chiropractic care is a logical approach, it is not a quick fix. Typically a lengthy course of care is recommended, with regular progress examinations to objectively evaluate changes.
-
Chen, Kao-Chang & Chiu, Elley. (2008). Adolescent Idiopathic Scoliosis Treated by Spinal Manipulation: A Case Study. The Journal of Alternative and Complementary Medicine: 14(6); 749-751.
-
Sanna, Mark. (2009). A New Look at Adolescent Idiopathic Scoliosis. The American Chiropractor: April 2009; 18-19.
-
Woggon, Dennis. (2005). Scoliosis Correction – CEAR Solutions; Chiropractic Leadership, Educational Advancement & Research. The American Chiropractor. February 2005; 54-56.
-
Hyland, John. (2008). Functional Scoliosis. The American Chiropractor. April 2008; 30-31
-
Payne, Mark. (2008). Scoliosis: A Postural Approach. The American Chiropractor. April 2008; 26-28.
-
Yochum, Terry & Maola, Chad. (2008). Scoliosis. The American Chiropractor. April 2008; 14-16.
-
Lamantia, Marc. (2009). Review of the Literature: Non-operative Scoliosis Treatment. The American Chiropractor. April 2009; 20-23.
-
Woggon, Dennis. (2006). Can Chiropractic Care Help Scoliosis? The American Chiropractor: May 2006; 24-25.
-
Morningstar, Mark, Woggan, Dennis & Lawrence, Gary. (2004). Scoliosis treatment using a combination of manipulative and rehabilitative therapy: a retrospective case series. BMC Musculoskeletal Disorders.